
UCL REPAIR WITH INTERNAL BRACE AUGMENTATION
'One of the best advancements in Tommy John Surgery in the past 40 years.' - Dr. Christopher Ahmad, Head Team Physician, New York Yankees
What is it and why?
UCL repair is a surgical technique that is different than Tommy John Surgery but can also correct an injured UCL. Rather than reconstruct or rebuild the ligament, the existing damaged ligament is repaired with high strength sutures. When the ligament is detachment from bone, the UCL is reattached with suture anchors. In addition, a collagen coated high strength tape is placed in a position to protect the repaired ligament. The major advantage of UCL repair when compared to Tommy John Surgery is the lengthy recovery time can be cut in ½ – 6 months in comparison to 12 months.
Am I a candidate for UCL repair with internal Brace?
- Dr. Ahmad will assess your UCL injury for potential UCL repair. The features on MRI can predict if the UCL can be repaired.
If you would like DR. Ahmad to review your MRI, click here. - The UCL injury that is most suitable for repair are discrete focal UCL tears with overall good quality to the ligament.
- UCL injuries that have significant tissue degeneration or calcification are considered relative contraindications to repair.
UCL Repair with Internal Brace Surgical Technique
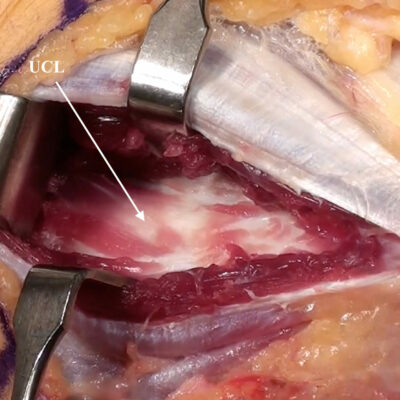
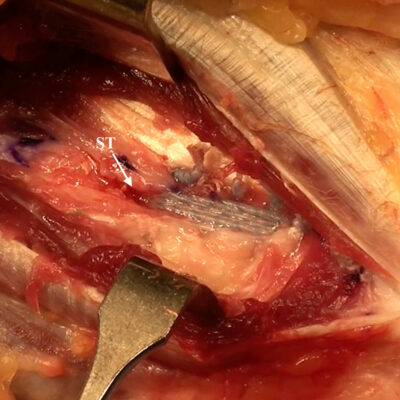
- The UCL is exposed and inspected for quality of tissue to confirm its ability to be repaired.
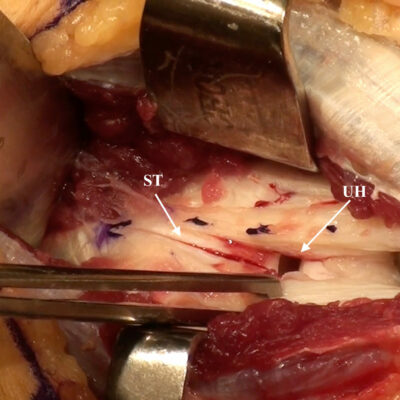
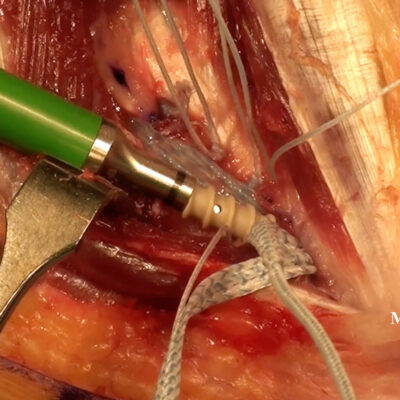
- Once confirmed that repair is appropriate, small 3.5 mm bone anchors loaded with collagen-dipped high-tensile strength tapes are placed into the ulna bone. The anchor is also loaded with a single 0 high-tensile strength suture that is passed into the torn ligament and tied for repair.
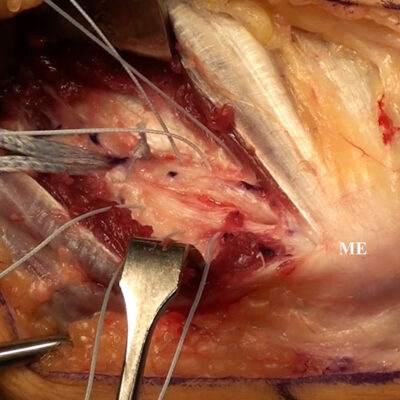
- The remainder of the native ligament is further repaired using interrupted 0 high-tensile strength non-absorbable sutures.
- The elbow is then held in position for final fixation of the internal brace.
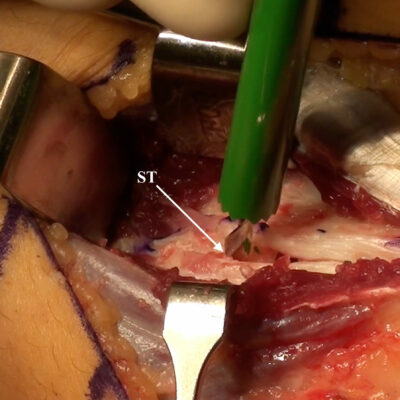
- The second anchor is prepared with a hole drilled into the humerus bone.
- The internal brace is then placed into the anchor. The anchor is inserted into the drill hole fixing the internal brace in optimal position.
- The elbow is then taken through a range of motion to ensure adequate isometry and tension of the internal brace.
Dr. Ahmad performs UCL repair with internal brace
REHABILITATION
- Rehabilitation following UCL repair with internal brace is accelerated by comparison to Tommy John Surgery
- Phase I (weeks 0 to 3): Splint for one week, then transition to a hinged elbow brace with gentle motion from 30° to 110° progressing to 10° to 125° at week 3. During this time, active ROM is started as well as light isotonic strengthening at day 10. The Thrower’s Ten Program is initiated toward the end of this phase.
- Phase II (weeks 4 to 8): Focus on enhancing mobility, improving strength, and regaining neuromuscular control. Brace is opened 0 to 145 at week 4. The advanced Thrower’s Ten Program is initiated along with a two-handed plyometric program starting in week 6. One handed plyometrics are started at week 8.
- Phase III (weeks 9 to 13): Advanced strengthening with an emphasis on a gradual return to sporting activities. For baseball players, a hitting program is begun at week 10 and a throwing program is started at week 11. The duration of the throwing program is variable, but most pitchers are able to progress to throwing from a mound after 10 weeks of progressive long toss. Throwing intensity is gradually increased off the mound, starting at 50% maximal intensity and gradually working up from there.
- Phase IV (weeks 14-26): Focus is on return to sport with emphasis on proper warm-up and a progressive return to competitive throwing.
Internal Brace Surgery