
Overview
What is Batter’s Shoulder ?
- Hitting a baseball is considered one of the most challenging tasks in sport and has unique injury patterns.
- Batter’s shoulder is an injury hitters suffer in the lead (front) shoulder due to the high-volume repetitive micro-trauma associated with hitting.
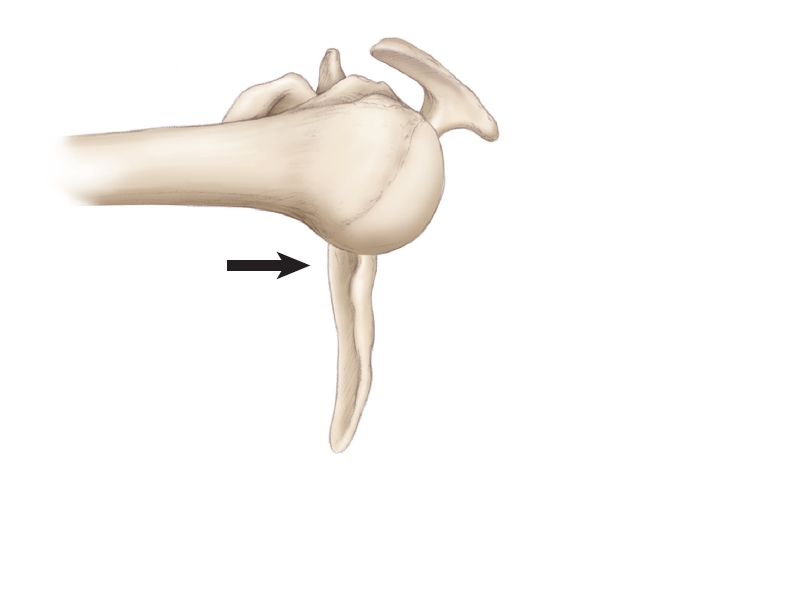
- The injury causes posterior labral tearing and posterior instability. (posterior is back part of shoulder)
Hitting Mechanics
- Hitting employs a kinetic chain sequence that is initiated in the legs.
- Tremendous force is generated in the larger lower half of the body that moves up through the core to the smaller shoulders, upper extremities and the bat itself.
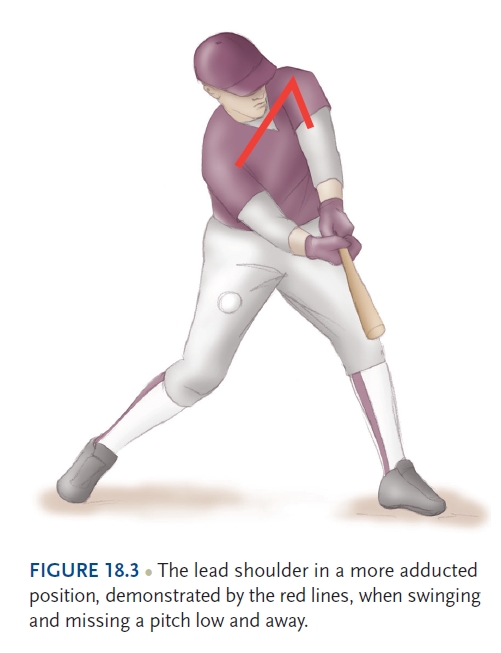
- The batter’s lead shoulder specifically experiences a posterior humeral head force with the arm positioned in relative adduction (adduction is shoulder coming across the front of your chest). Shoulder adduction is increased when a player swings at pitch that is on the outside portion of home plate.
- Whereas the majority of position players throw right handed, switch hitters and left-handed batters are of special interest since their lead hitting shoulder experiences the additional stress of throwing. Hitting related shoulder injuries can therefore create throwing related symptoms and corrective posterior instability surgery needs to avoid overtightening the posterior capsule.
Hitting Kinetic Sequence
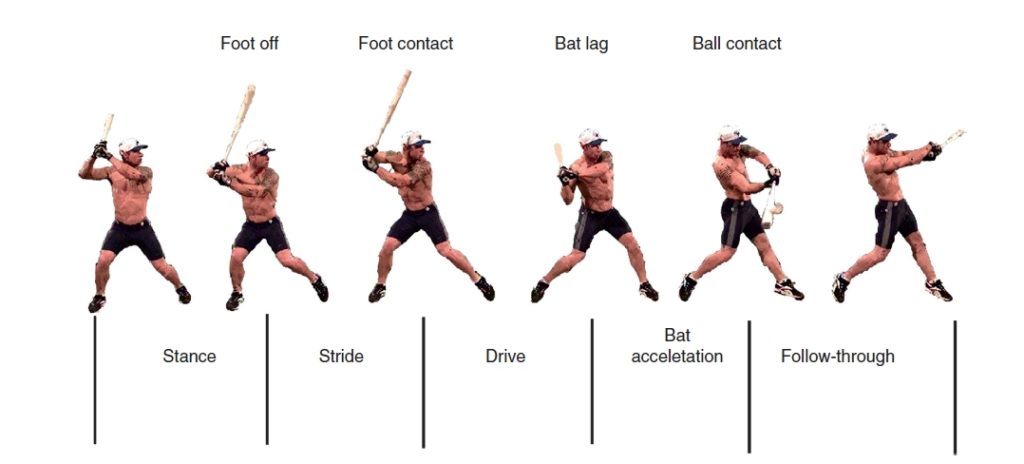
- The hitting motion can be broken into five different phases (Figure 18.1). The process of hitting is initiated when there is front foot elevation. During this phase, weight is transferred to the back leg. Also, the hips, trunk, and upper body begin coiling. The coiling phase is where the body rotates away from the approaching baseball. The lead shoulder is in maximum internal rotation and adduction during the coiling phase.
- At foot contact, upper body uncoiling begins. As the hips rotate towards the ball the trunk remains relatively neutral and the shoulders continue towards maximum rotation. The upper extremities begin their rotation forward as the trunk rotates towards the ball in an attempt to maximize the angular velocity of the bat as it approaches ball contact. This process of the hitter initiating his swing to the point where his bat crosses the plate is about 0.2 seconds.
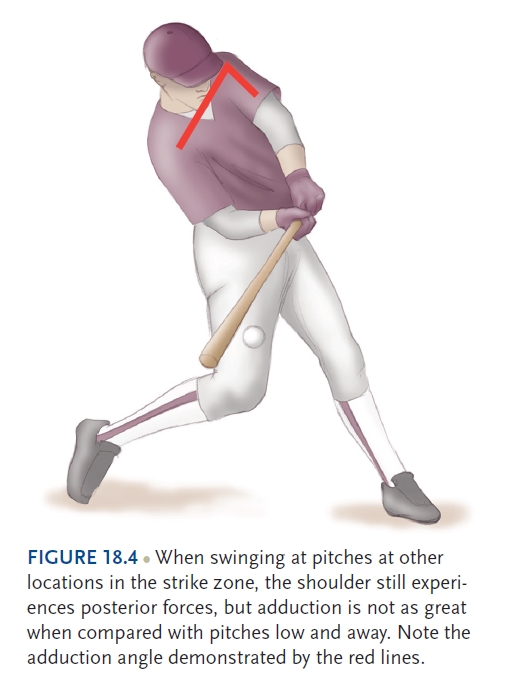
- Throughout the hitting motion, much of the force generated in the batter’s shoulder is over the posterior portion of the lead shoulder. Just prior to ball contact, there is over 500 pounds of force directed posteriorly on the shoulder. As the activity of the posterior deltoid increases during acceleration of the swing, large forces are directed upon the humeral head. The humeral head is already in a posteriorly directed position as it is adducted and internally rotated. Forces may change depending on pitch location. The front shoulder is more adducted and flexed during a swing on an outside pitch compared to swings taken on an inside pitch.
- If the player makes contact, kinetic energy from the bat is transferred into the ball and additional stabilizing muscles are recruited, dissipating the total amount of energy the body must stop during the follow-through. If the player swings and misses, they must stop the energy of the bat during the follow-through. The lead shoulder does most of the work in slowing the bat down during a follow-through on a missed pitch and the stresses placed on the posterior shoulder may be increased due to the lack of recruited stabilizing muscles.
- As the bat moves towards the front of the batter, there is an increased posteriorly directed force that can exceed the ability of the labrum and capsule containing the humeral head. This can lead to posterior subluxations of the humeral head, damaging the posterior labrum and other tissues. The follow-through also stresses the anterior capsule and labrum especially when the player finishes their swing one-handed.
What does a hitter with batter’s shoulder feel?
- Hitters often feel the ball and socket disconnect with the ball shifting out of the socket during a swing-and-miss or reaching for an outside pitch.
- Hitters then experience pain, and apprehension with swinging at pitches that are outside, typically low-and-away (Figure 18.3), or up-and-in (Figure 18.4).
- Symptoms are exacerbated by swinging and missing since no energy is dissipated to the ball.
How Does Dr. Ahmad and his Team make the Diagnosis?
- Ahmad and his team will perform a comprehensive physical examination.
- Specific tests of the posterior labrum include the load and shift the shoulder joint to see of the ball shifts out of the socket. (Figure 18.3A Figure 18.3B).
- One or all of these special tests may be considered positive when pain is elicited or a clunk or click is felt or heard. MRI
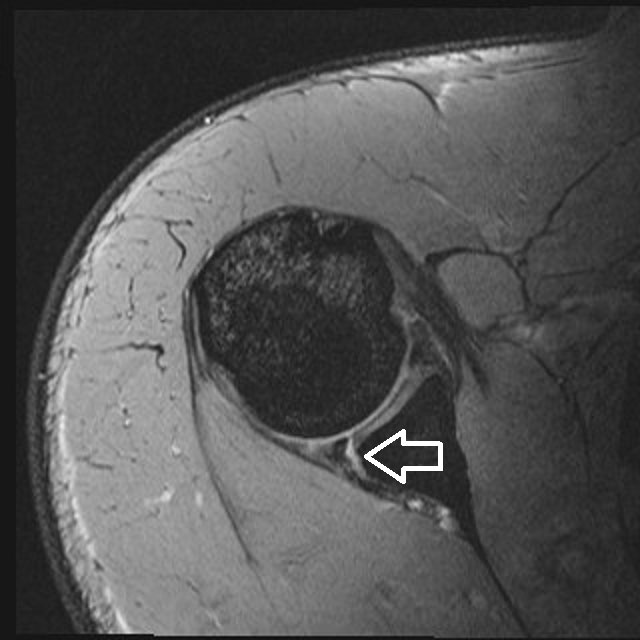
- Ahmad and his team will obtain Magnetic resonance imaging (MRI) which generally demonstrates a posterior labral tear (Figure 18.4 A).
- MRI may also help depict any additional pathology such as a chondral lesion (Figure 18.4 B).




Treatment Options
Non-Operative Treatment
- Non-operative treatment of the batter’s shoulder can be tried. Players undergo a period of complete rest from swinging. Physical therapy re-establishes shoulder range of motion, improving rotator cuff and peri-scapular muscle strength. Once symptoms are alleviated, a swing progression is initiated with an emphasis on proper mechanics.
- Should the lead shoulder and throwing shoulder be the same, return to throwing and hitting should be staggered. This will help alleviate the amount of stress put on the shoulder simultaneously and prevent a setback. A non-operative approach may take as long as 12 weeks.
Operative Treatment
- Surgical intervention is indicated with failure of non-operative treatment. However, some athletes may wish to avoid failure of non-operative treatment and elect for earlier surgical intervention based on seasonal and career timing.
How does Dr. Ahmad surgically correct Batter’s Shoulder?
Surgical Technique Step by Step
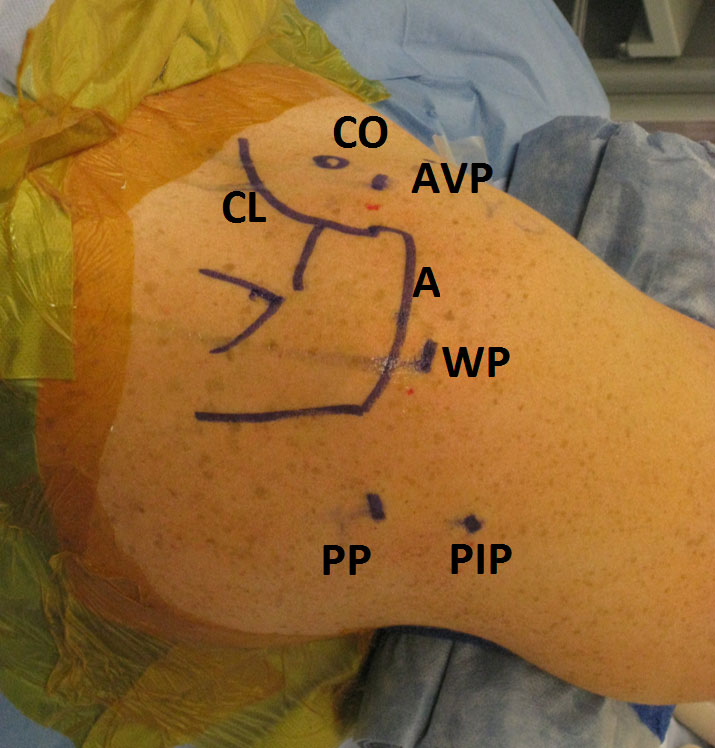
- Shoulder anatomy is outlined on the skin.
- The arthroscope is initially placed in the back of the shoulder.
- Diagnostic arthroscopy evaluates the entire labrum as well as the rotator cuff.
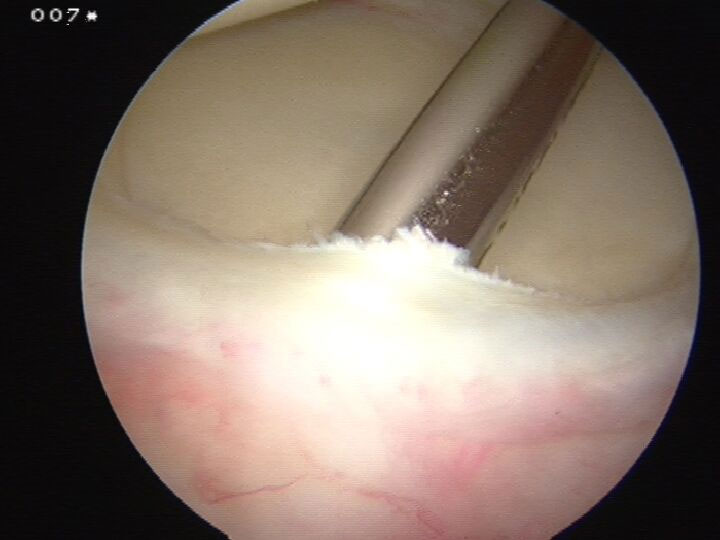
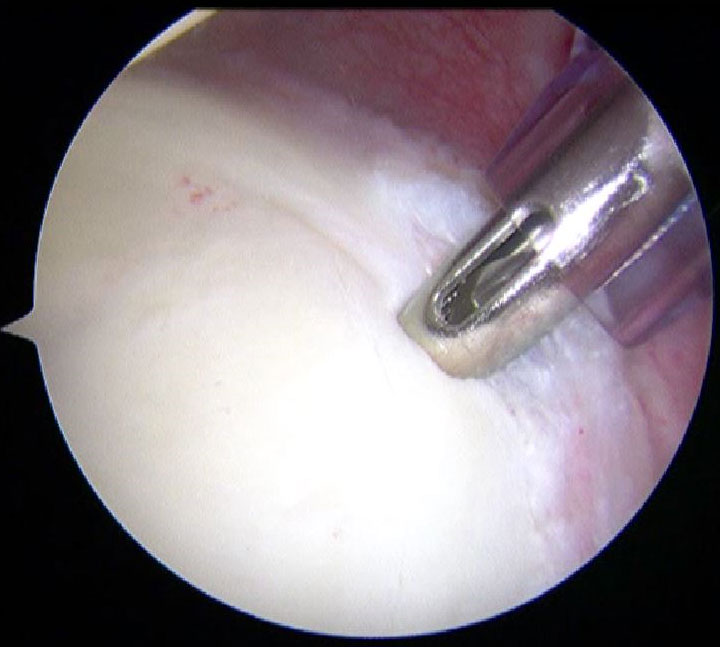
- An incision is made in the front of the shoulder and a probe is introduced and used to assess the integrity of the labral attachment to the glenoid (Figure 18.6). Any undersurface rotator cuff partial tearing is debrided. The scope is placed into the front cannula and the back of the shoulder injured capsulolabral complex is better visualized.
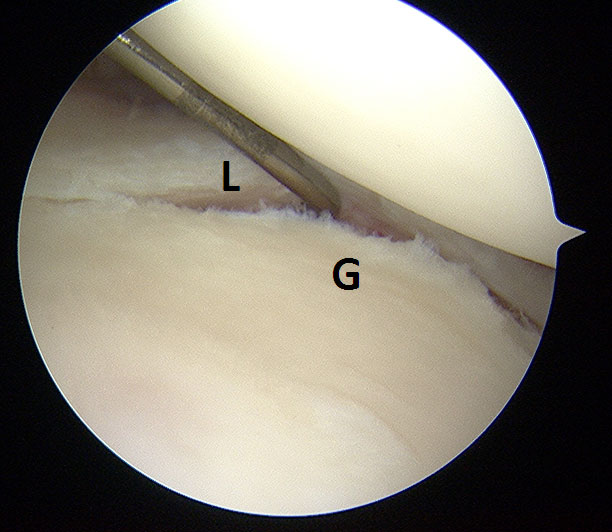
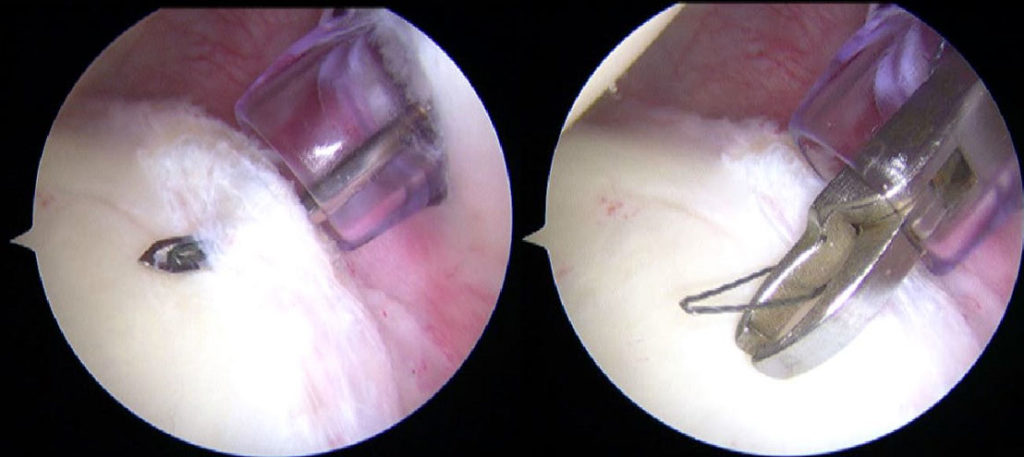
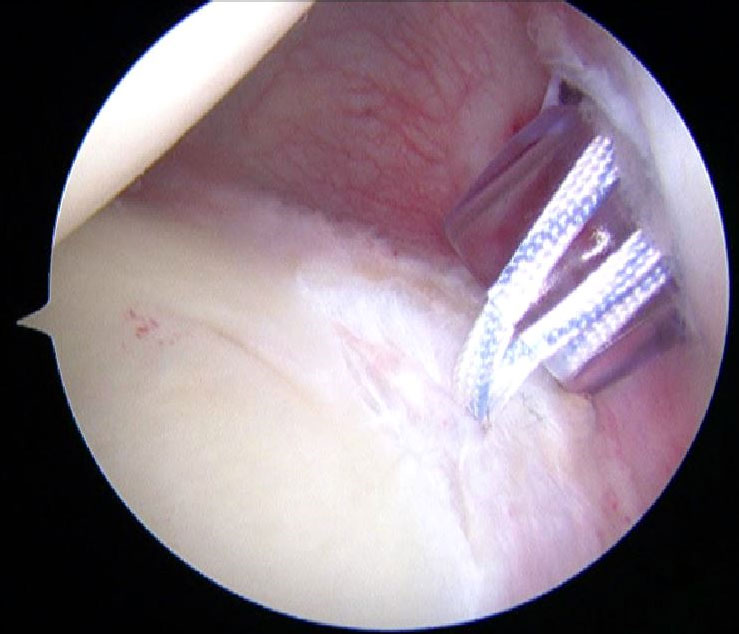
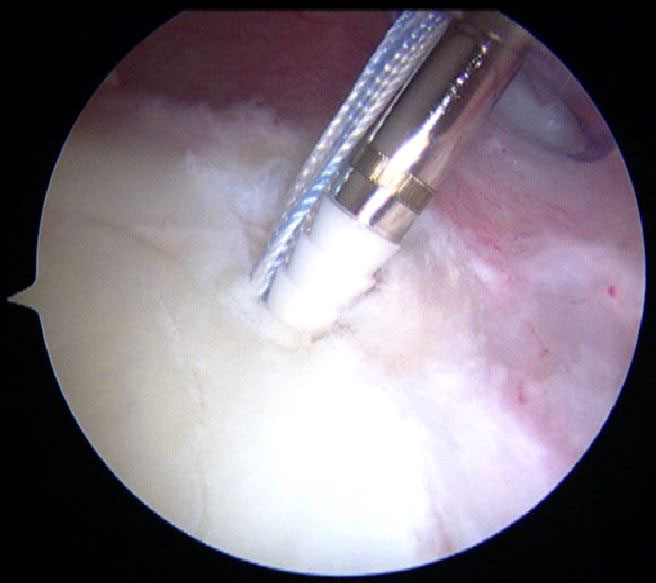
- All labral tissues requiring repair are mobilized and adjacent glenoid surfaces are abraded with a shaver or rasp to enhance healing (Figure 18.7). A percutaneous approach allows placement of suture passing devices to suture tape around the capsulolabral complex. The extent of capsule incorporated in the repair depends on the degree of instability. If the lead shoulder is also the throwing shoulder, then overtightening the capsule is avoided. A drill guide and drill are used to create a hole at the articular margin of the glenoid. The suture tape is placed through the eyelet of the anchor. The anchor is then placed in the predrilled glenoid hole and tension is applied to the tape (Figure 18.8). The anchor is inserted securing the tape and excess tape is cut. The suture passing and fixation process is repeated to complete the repair (Figure 18.9).
What is the Post-Surgical Rehabilitation?
- The player is immobilized in a sling with slight external rotation, which will be used for 6 weeks. The sling may be removed throughout the day only for light daily activities. Physical therapy is initially aimed at restoring range of motion while avoiding posterior stress. Once range of motion is restored, resistance training and plyometric exercises are initiated.
- A return to hitting program is initiated 4 months post-operatively. Should the lead shoulder and throwing shoulder be the same, a throwing program is initiated at 4 months and a hitting program is delayed. This delay is built-in to the player’s rehabilitation program as to not over-stress the repaired labrum. Once a return to play is initiated, it is suggested that players continue to maintain the strength of the rotator cuff.
- Return to hitting begins on a tee. Once the player successfully completes a phase of hitting off a tee, he may progress to soft-toss and live batting practice. Should a throwing program be necessary, it should be initiated 6 weeks after the hitting progression begins. Players may return to competition at 5 to 6 months postoperatively although timelines vary for each patient.
Summary
- Batter’s Shoulder affects the lead shoulder of the batter.
- Greater consideration for avoidance of overtightening the posterior shoulder is required for players whose lead hitting and throwing shoulder are the same so throwing related symptoms are avoided.
- Initial treatment should be non-operative but surgical treatment may be elected earlier due to seasonal and career timing.
- Operative treatment is indicated after failure of non-operative treatment.
- A knotless technique is preferred.
- Players return to Live Hitting around 5 to 6 months postoperatively.