
Accurate Diagnosis of a Tommy John Injury
Did you Injure your UCL?
This is how Dr. Ahmad and his Team will accurately diagnose your Elbow Injury.
For players who have a suspected UCL injury, accurate and immediate diagnosis is critical. Delayed or missed diagnosis could, and often does, result in time away from playing which could have been avoided. Gathering information is a large part of establishing a player’s diagnosis and includes a physical exam and an MRI.
Factors that help establish treatment are severity of injury; presence or absence of additional injuries, such as bone spurs, loose bone chips, calcification within the UCL, forearm flexor tendon tears or strains, ulnar nerve compression or subluxation, bone stress fractures or stress reactions; seasonal timing, and the player’s desire to continue playing.
Signs and Symptoms – What to Look Out For
- Pain localized to inside elbow (location of the UCL) during throwing or after throwing. (figure here)
- Stiffness where elbow is hard to bend or extend.
- Tight feeling in the forearm muscles
- Numbness or tingling the ring and pinky fingers
- Difficulty warming up
- Decreased velocity
- Loss of command
UCL injuries can encompass a spectrum of symptoms. On one end, a player may feel a sudden pop and acute pain during a game and will be unable to continue throwing. On the other end of the spectrum, a patient may simply have progressive loss of accuracy difficulty loosening up, and diminishing velocity.
The injury most commonly afflicts high-level athletes involved in intense throwing. Dr. Ahmad and his team ascertains the position, competitive level, and future aspirations of athletes who have injured their UCL to determine best individualized treatment. It’s also important to know if the player had a sudden difference in the volume of throwing, velocity, or pitching mechanics. Dr. Ahmad and his team will also assess problems with their hip, leg, or core function, such as injury or inflexibility that could contribute to their injury. Patients who injure their UCL have various symptoms.

Patient example 1
JT is 16 yo HS baseball pitcher with aspirations of playing in college. He participated in several show cases during the summer and his velocity was increasing as he was also putting on muscle mass. During a show case, he felt a sudden pain in the inside of his elbow while throwing a fastball. He was unable to continue throwing. He developed numbness in his pinky and his elbow became stiff within a few hours and he was unable to fully bend his elbow. Subsequent evaluation in the office including physical examination and MRI scan revealed a UCL tear.
Patient example 2
AJ is a 24 professional pitcher. He pitched 2 innings in a game and felt fine. 2 days later he tried to play catch and his elbow felt stiff and took him longer to loosen up. He pitched again and noted his velocity was down and his command was poor. His elbow became stiff and he again experienced difficulty warming up and playing catch 2 days later. He subsequently underwent a physical exam and MRI and high grade partial tear of his UCL was identified.

Physical Examination
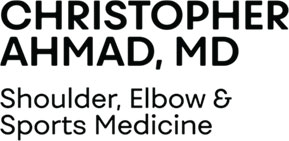
Dr. Ahmad and his team will perform a physical exam in the office. The inside aspect of the elbow it typically demonstrates tenderness over the ligament. Some players may even exhibit swelling over the medial elbow as well. Range of motion may be limited in both flexion and extension. (Figure – elbow tenderness with silhouette of ligament anatomy under the skin). The hallmark test to indicate a ligament tear is called the moving valgus stress test. The examiner stabilizes the elbow against an exam table and puts subtle stress across the arm, which pulls on the UCL. Patients with a UCL tear experience pain as the elbow is flexed and extended.
Players who have bone spurs typically lack full extension. Dr. Ahmad will also assess possible associated injuries including bone spurs, ulnar nerve compression or instability, stress fracture or stress reaction, or muscle strains. These players also have pain with special tests called the bounce test and arm bar. If players exhibit persistent numbness and tingling and have a positive Tinel’s sign. Players will also have their shoulder, hips and core evaluated.
UCL Stress Testing
Imaging Studies – X-rays, MRI, and ultrasound
Patients with a suspected UCL injury typically undergo x-rays as the initial imaging study. X-rays may demonstrate calcification in the UCL, loose bodies, bone spurs, or stress fracture.
To diagnose a UCL injury accurately, an MRI enables detection of partial thickness tears or full thickness tears and other possible injuries such a flexor muscle strain. Occasionally, an MR Arthrogram is recommended if an MRI is inconclusive. An arthrogram uses contrast dye is injected into the elbow to better visualize possible small UCL injuries.
Dr. Ahmad frequently performs ultrasound evaluation of the UCL in the office. Ultrasound offers immediate availability (ultrasound is at every office location), does require any expense or insurance authorization, and can be used to test the function of the UCL. When the elbow has stress applied to it, an intact UCL will keep the joint stable whereas a compromised UCL (either torn of stretched) will allow the joint to gap open.





Dynamic Ultrasound Diagnosis of UCL Injury
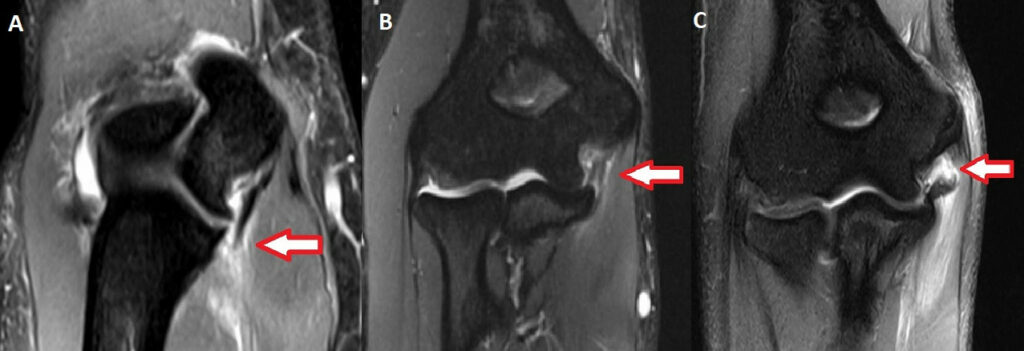
MRI determines UCL injury characteristics that influence healing capacity.
A number of features influence prognosis for non-operative vs operative treatment of UCL injuries. First is the severity or degree of tear. Full thickness tears in which all the fibers of the ligament are torn have less healing capacity than partial tears. Partial tears can occur in varying degrees of severity. Edema, or swelling, surrounding the ligament also can indicate more severe injury. Many players who have sustained a partial UCL tear commonly hear the degree of tear associated with a percentage. For example, a player may say he has a 50% partial tear.
The location of the tear also influences healing. Tears that occur at the bottom (distal) portion of the ligament have less healing potential than tears at the top (proximal) part of the ligament. Finally, some ligaments have undergone prior injury and healing which is suggested by the existence of calcification or thickening of the ligament. A small acute tear on a ligament with chronic changes has less healing potential than a small acute tear on a normal ligament.