
Overview
The medial epicondyle is an important structure in the elbow. It is the knob on the inside part of our elbow and serves as an attachment site for various muscles, tendons, and ligaments. The flexor muscles which help us flex and pronate (turn our palm to the ground) our wrist attach to the medial epicondyle. In throwers, the ulnar collateral ligament (UCL) originates at the medial epicondyle and inserts at the sublime tubercle on the ulna. At the posterior aspect, the ulnar nerve runs through the cubital tunnel and supplies feeling to the inside part of our elbow, as well as the pinky and ring fingers. Young throwers that are still growing have an increased risk of injuring the growth plate at the medial epicondyle.
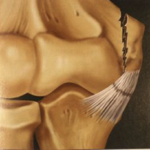 The epicondyle can become injured in a number of different ways. In some cases it may become fractured due to direct trauma. In young baseball players, the development of Little Leaguer’s Elbow and insufficient rest may result in a medial epicondyle avulsion fracture. The valgus stress of throwing that is sustained across the medial elbow is tremendous.The muscles and ligaments pulling on the epicondyle may lead to an avulsion fracture because the UCL is stronger than the bone it attaches to. An avulsion fracture is where the muscle or ligament pulls the attachment site of the bone away from its origin.
The epicondyle can become injured in a number of different ways. In some cases it may become fractured due to direct trauma. In young baseball players, the development of Little Leaguer’s Elbow and insufficient rest may result in a medial epicondyle avulsion fracture. The valgus stress of throwing that is sustained across the medial elbow is tremendous.The muscles and ligaments pulling on the epicondyle may lead to an avulsion fracture because the UCL is stronger than the bone it attaches to. An avulsion fracture is where the muscle or ligament pulls the attachment site of the bone away from its origin.
Fractures of the medial epicondyle are one of the more common fractures seen in pediatric patients and is on the rise due to athletic demands. Pediatric patients are generally between the ages of 11 and 14 and participate in overhead or throwing sports.
SYMPTOMS
Young baseball players, especially pitchers, may experience an acute injury on a single throw.
- Popping sensation
- Immediate pain
- Inability to continue throwing
- Tingling sensation in pinky and ring fingers due to nerve irritation
What to expect when you see Dr Ahmad
Dr. Ahmad and his team will take an extensive analysis including past medical and athletic participation histories.
- Review details of your child’s injury
- Elbow assessment
- Review X-rays and MRI/CT scans
Physical Exam and Imaging
 Diagnosis is confirmed after comprehensive evaluation.
Diagnosis is confirmed after comprehensive evaluation.- Physical evaluation is comprised of the medial elbow and related structures.
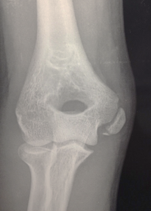
- X-ray imaging is required to correctly diagnose a medial epicondyle fracture. In some cases, an X-ray of the uninjured elbow may be required for comparison.
- MRI scan may also be recommended to evaluate muscular, tendon, or ligament injuries.
- CT scan may be used to further assess the fracture.
 Diagnosis is confirmed after comprehensive evaluation.
Diagnosis is confirmed after comprehensive evaluation.Treatment Options
Treatment of medial epicondyle injuries, regardless of etiology, can be treated non-operatively or with surgery.
Non-surgical
For injuries that have not displaced the bone and the bone maintains anatomic, or good, positioning in the elbow then non-operative treatment can be elected.
Treatment includes:
- Bracing that immobilizes the elbow.
- Physical Therapy once healing is observed on repeat x-ray imaging
- Return to Throwing Program when healing and strength are sufficient
- Unrestricted return to play restriction at successful completion of the throwing program

Surgical
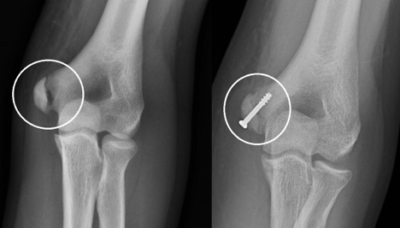
For patients that has a displaced avulsion fracture, surgery is indicated.
Surgery includes:
- Open reduction and internal fixation of the broken bone
- An incision is made at the medial elbow to visualize the fractured piece
- Screw placement into the fragmented piece and reattached to the humerus
- The patient is placed in an elbow brace for 6 weeks
- Physical Therapy is initiated followed by a throwing program
- Unrestricted return to play at successful completion of PT and throwing programs
Goal of Surgery:
- To reposition the bone back to its normal position
- Ensure healing of the bone
What happens if there is a delay in diagnosis or a delay in treatment?
Unfortunately, Dr. Ahmad sees several patients each year who have had a delay in diagnosis or a delay in treatment. This often results in what is referred to as a nonunion.
- Nonunion
- The bone fails to heal
- It becomes scarred in an abnormal location
- Results in pain and inability to get back to throwing
- Challenging situation but can be corrected with surgery.
- Surgery involves
- Removal of extensive scar tissue
- Mobilizing the bone fragment back to its normal position
- Fixing it with screws
- In general, it is better to surgically fix epicondyle fractures in young athletes who wish to continue playing baseball early before nonunion occurs

Case example of a nonunion and a high school football quarterback. X-rays show that the initial surgery did not work. Subsequent surgery by Dr. Ahmad achieves healing of the bone and the athlete returns to full playing.