
Overview
- Medial epicondylitis or “golfer’s elbow” represents pathologic changes to the forearm muscles attachment to the inside aspect of the elbow. The tendon attachment demonstrates inflammation in its mild form progressing to actual tearing in its severe form.
- The repetition of forceful muscle contractions contributes to the development of this condition.
- The incidence of medial epicondylitis is 5 to 20 times less common than lateral epicondylitis (tennis elbow) and is therefore often not diagnosed accurately.
Who is affected by golfer’s elbow?
- Pain develops on the inside part of the elbow.
- The pain is worse with gripping activity where the wrist and elbow are extended.
- The condition is common in golfers, baseball players, weightlifters, and bowlers.
- Laborers who use heavy tools
- Anyone engaging in repetitive gripping or lifting tasks
- Most commonly seen in patients between the ages of 35 and 50
Symptoms:
- Pain develops on the inside part of the elbow.
- The pain is worse with gripping activity where the wrist and elbow are extended.
- Discomfort or pain with holding objects such as a gallon of milk.
Physical Exam and Imaging
Dr. Ahmad and his team meet with each patient to discuss their symptoms and any relevant history. Dr. Ahmad then performs a physical examination, including range of motion and special tests, to further confirm the diagnosis. In some situations, an MRI scan may be ordered to determine the severity of the epicondylitis.
What to expect when you see Dr Ahmad

Yellow arrows showing significant tendon tear.
- Diagnosis is confirmed after evaluation
- Physical exam is comprised of the medial elbow and related structures
- X-ray imaging is used to determine the status of the bony anatomy
- MRI aids in determining the severity of the medial epicondylitis.
- MRI detects tendon tears or signal changes related to tendinopathy.
Treatment Options
Treatment of medial epicondylitis is dependent on a number of factors including duration and severity of symptoms. Patients may elect for non-operative or surgical treatment based on evaluation and shared decision making with Dr. Ahmad and his team.
Non-surgical
- First treatment step, successful for many
- Eliminate the activities producing pain
- i.e., lifting weights, intense gripping
- NSAIDS and a rehabilitation protocol
- Decrease inflammation, icing, compression wrap
- Physical therapy should focus on eccentric strengthening
- Some patients elect to use a tennis elbow brace during the day or with activities
Injection Treatments
- May be used if oral NSAIDs do not help
- 2 different types: Cortisone and Platelet-Rich Plasma (PRP)
- Cortisone helps to alleviate any inflammation right at the source
- PRP is used in the treatment of more severe medial epicondylitis
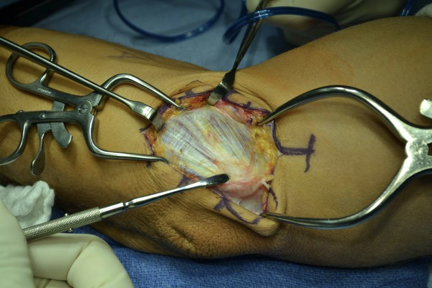
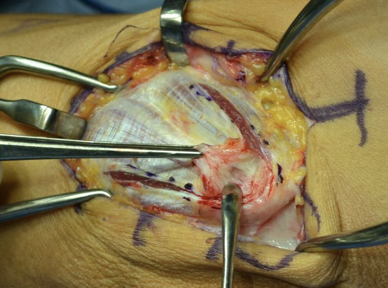
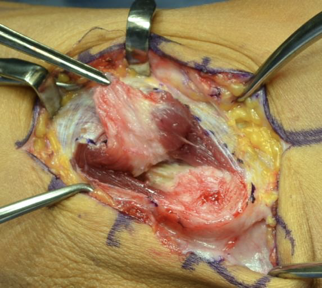
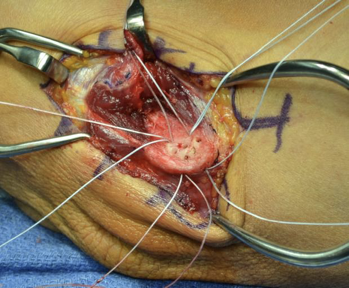
Operative Treatment
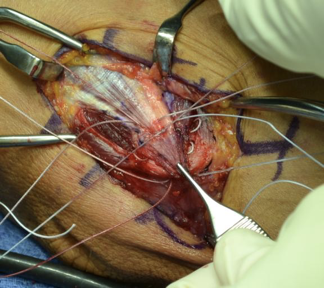
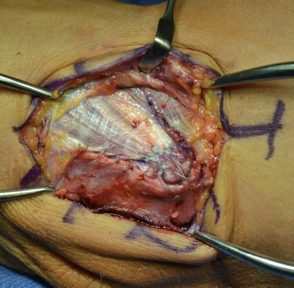
- Open Debridement
- Small incision allows Dr. Ahmad to visualize the damaged tissue
- Damaged tissues is removed and healthy tissue is repaired
- Recovery
- Sling for 24 hours
- Wrist splint for 4 to 6 weeks (varies on severity of epicondylitis). Occasional an elbow brace is used.
- Physical therapy helps decrease swelling, pain, and to regain strength in extensor muscles
- Avoid gripping activities such as opening a jar or lifting objects greater than 3 pounds.