
Overview
One of the more serious knee injuries an athlete can sustain is a tear of the anterior cruciate ligament, more commonly known as the ACL. Tearing of the ACL is usually seen in athletes playing high-contact or collision sports—however this is not a requirement for the injury. An ACL tear usually occurs when an athlete plants their foot, and twists, usually hearing a popping sound in their knee at the time of injury.
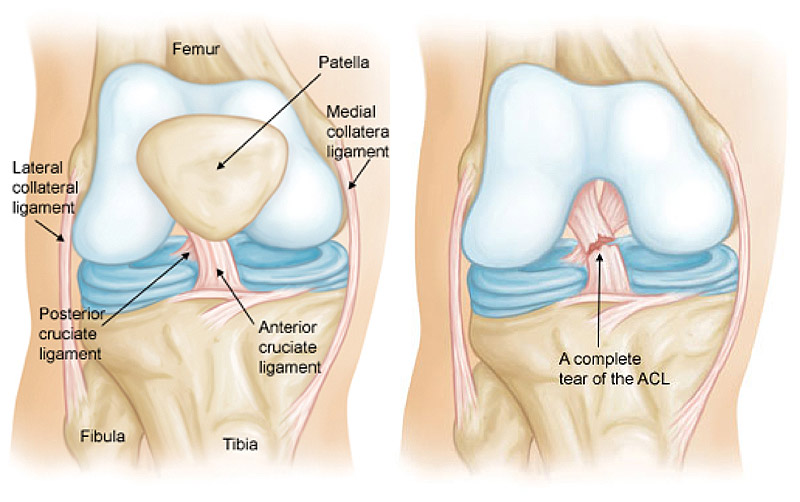
When the ACL is torn, another injury may be present, such as a torn meniscus and/or medical collateral ligament (MCL), a torn lateral collateral ligament (LCL), or a torn posterior cruciate ligament (PCL).
An ACL is: A cruciate ligament of the knee that attaches the front of the tibia with the back of the femur and functions especially to prevent hyper-extension of the knee.
An MCL is: A collateral ligament on the inside of the knee that serves as a stabilizer for the joint and supports the function of the knee.
The Facts on ACL Injuries:
ACL tears can occur in both males and females, but are more likely to occur in females Tearing an ACL usually involves planting of the foot and twisting A popping sound is commonly heard at the time of injury.
What Causes ACL Injuries:
- Quickly pivoting
- Suddenly stopping or slowing down while running
- Landing from a jump incorrectly
- Direct contact or collision, such as a football tackle or being slide tackled in soccer
Symptoms:
These are the most common symptoms of an ACL Injury:
- Pain
- Swelling
- Loss of full range of motion
- Tenderness along the joint line
- Discomfort or pain while walking
- Feeling of instability
In some cases swelling and pain could resolve on its own within 24 hours. However, if an attempt to return to play is made, the knee could be unstable causing an increased risk of injuring other structures in the knee.
Evaluation by Team Ahmad
Dr. Ahmad and his team of health professionals will greet you and start your visit with a discussion of your injury and symptoms. Next, the doctor will exam your affected knee, focusing on:
- Your history with sports and knee issues
- Pain points and reported levels of pain
- The range of motion of each knee
- The structure of both knees
Often, Dr. Ahmad will request an imaging scan, like an MRI to determine the extent of any soft-tissue damage.

Treatment Options
If you are experiencing intense knee pain or feelings of instability, you may require treatment to repair and prevent any further damage. You should cease all strenuous activity and make an appointment with your doctor immediately.
Surgical
Depending on the severity of the injury of your ACL, Dr. Ahmad will either recommend that the ligament be repaired or reconstructed. If the tear of the ACL is not complete, then Dr. Ahmad will recommend the ligament be repaired. If the ligament tear is complete, reconstructive surgery will be required.
Surgery itself takes roughly an hour, and afterward you will be in the post-anesthesia care unit (PACU) for 2 to 3 hours depending on how you react to the anesthesia. Crutches and brace are used after the operation and, in most cases, patients will be allowed to weight-bear as tolerated; meaning that you can put as much, or as little weight on the knee as you can tolerate.
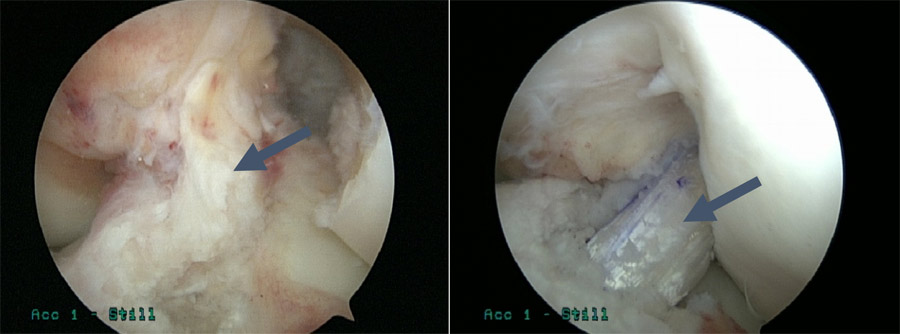
ACL Tear (Left) and ACL Construction (Right)
ACL Reconstruction:
- An ACL reconstruction is performed when the ligament is completely torn.
- The surgery is performed at an out-patient setting where the patient comes in, has surgery, and goes home in the same day.
- Dr. Ahmad performs an ACL reconstruction arthroscopically, making two small incisions on both sides of the patella to pass the camera (arthroscope) and other instruments into the joint.
- Patients usually require three types of grafts to reconstruct the ACL. Typically, another incision is made where the graft is taken.
- Two are called autograft (where the tissue is taken from the patient’s own body).
- The third is called an allograft(tissue comes from a donor and is treated so it is safe for a recipient to use).
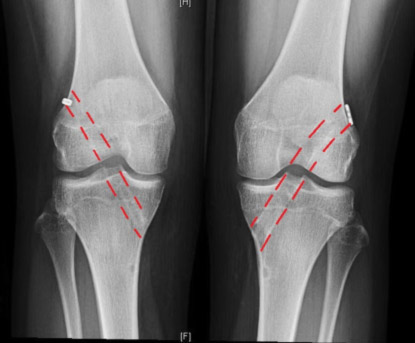
Post-operative X-rays of the tunnels in a patient with bilateral ACL reconstructions done by Dr. Ahmad.
ACL Repair
- When the ACL is not completely torn, a repair may be possible.
- Surgery is performed at an out-patient setting where the patient comes in, has surgery, and goes home in the same day.
- ACL repairs are performed arthroscopically, where two small incisions are made on both sides of the patella to pass a camera (arthroscope) and other instruments into the joint.
- To repair the ACL, Dr. Ahmad sutures the ligament to the attachment site.
- This innovative procedure is just as effective as a reconstructive operation.
Rehabilitation and Recovery
Phases of Rehabilitation
- In some cases prehab will be necessary to decrease swelling and increase range of motion prior to surgery.
- After surgery, physical therapy focuses on regaining quad control, restoring range of motion, and decreasing swelling.
- Low-level strength training is through exercises such as quad sets, straight leg raises, and flexion exercises.
- As range of motion improves, strength training is introduced to help protect the new ligament.
- As strength increases, more stress will be applied to the ligaments and muscles of the knee.
- The final phase of rehab is aims for a successful return to play tailored to the athlete’s sport.
Return to Sports
The rehab process is a gradual progression leading up to a return to play. There are a few milestones along the course for each athlete to reach prior to making their return to play.
At the 3 month mark, athletes are allowed to begin running straight ahead
Around post-op month 4, more sport specific drills come into play
At 6 months athletes are allowed to perform sport-specific tasks with an opponent on them (such as dribbling a soccer ball past an opponent or taking a basketball shot against a defender)
When getting ready for a return to play, Dr. Ahmad recommends the use of a custom brace for at least a year after surgery
*Note: All timelines are meant as a guide, your actual timeline may vary.*
Patient Stories

Alexander Ciccone – ACL / MCL Tear
I was playing for a Division 3 university when the unexpected happened. During a routine workout session with...


The Model Brothers – Anterior Cruciate Ligaments
At ages 14 & 15, Max and Cole saw Spikeball on Shark Tank and decided to play in...